MRI NEWSLETTER: Traumatic TFC Tear
Posted May 8, 2018
Palmer divides triangular fibocartilage (TFC) tears into traumatic and degenerative. The Palmer 1B tear is a traumatic tear of the peripheral attachment of the TFC on the ulnar side with a styloid or foveal attachment (or both) tear. The foveal attachment is most important to DRUJ stability.
The triangular fibrocartilage (TFC) disc is a major stabiliser of the distal radial ulnar joint. The TFC disc attaches directly on the articular cartilage of the radius. On the ulnar side, the TFC disc has two attachments: the proximal lamina which attaches to the foveal ulnaris and the distal lamina which attaches to the ulnar styloid. These two attachments of the TFC disc on the ulnar side are sometimes called the triangular ligaments.
This is important because some surgeons in the last few years have begun reattaching the foveal component of the TFC to increase stabilisation of the DRUJ.
Tears of the peripheral triangular fibrocartilage (TFC) result in clinical DRUF instability resulting in ulnar sided pain, reduction of grip strength, and reduced rotation of the forearm. The wrist gives way while turning a steering wheel or opening a bottle.
The foveal attachment is necessary for DRUJ stability. Radiologists must evaluate the foveal attachment.
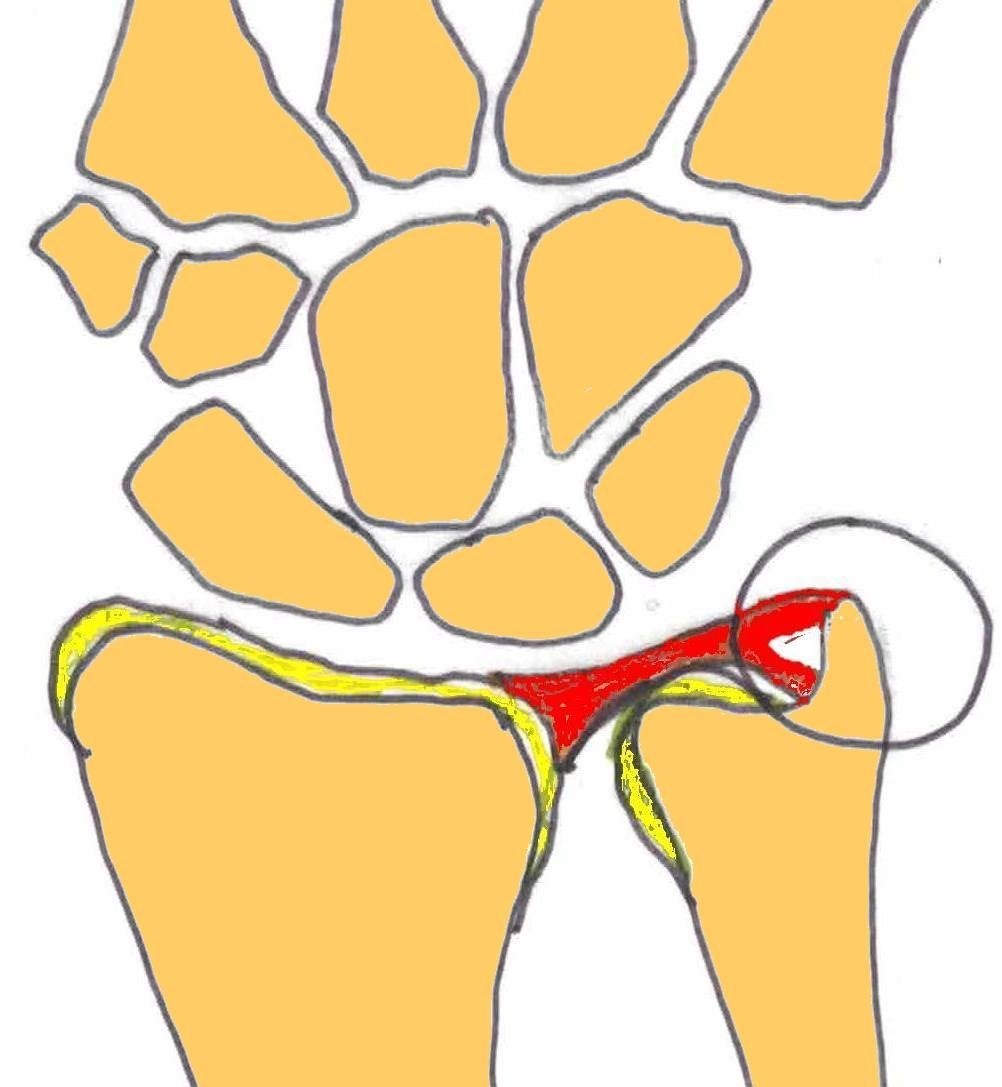
Diagram of the Complete 1B TFC Tear
Both the foveal and styloid attachments are torn so contract injected into the radiocarpal joint would extend into the DRUJ
1B Tear: tear of the proxima lamina (foveal attachment) Partial Tear
If the radiocarpal joint is injected, no contrast will extend into the DRUJ; therefore, this is called a non-communicating partial tear. In order to visualise the foveal tear, the DRUJ is injected and an MR exam is performed. On the DRUJ injection, the torn fragment of the foveal attachment can be identified.
Read the full article here: Traumatic TFC Tear
By Dr William Renner